

This year d-wise has worked with multiple clients to prepare and submit collaborative EMA and Health Canada submissions. Here are ten takeaways from our experience.
As we progress towards increased data publication across the globe, transparency teams will be looking for the safest, most efficient ways to handle clinical data publication for multiple regulatory agencies. We believe that collaboration when publishing globally is key. Global harmonization not only reduces duplicate efforts on behalf of the sponsor, it also minimizes risk of re-identification and helps to build public trust through consistency. EMA and Health Canada have been working with sponsors submitting data during this time, and we hope they continue to do so – the two agencies released a promising statement about collaboration earlier this year.
This year, d-wise has worked with multiple clients to prepare and submit collaborative EMA and Health Canada submissions. Throughout our submission preparations we found opportunities for alignment and efficiency as well as some areas that could not be combined due to system or process dependencies.
Here are our ten takeaways from the collaborative submission process:
1. Plan Ahead for Shortened Timelines
While the process remained the same, the timelines were significantly consolidated for our first collaborative submission. For comparison, a typical EMA submission cycle takes up to 120 days. Our first collaborative submission cycle was completed in two weeks.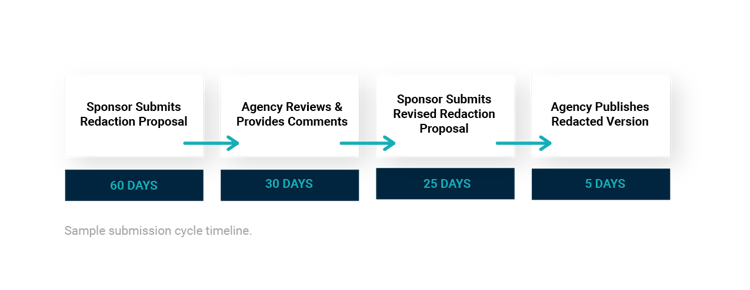 For concurrent submissions, both Health Canada and the EMA aim to have comments back to the sponsor within 2 weeks. If their timelines align, there’s a chance that comments will come back from both agencies at the same time. The EMA has also requested that the draft anonymization report is shared before starting anonymization so they can come to an agreement on the approach with the sponsor.
For concurrent submissions, both Health Canada and the EMA aim to have comments back to the sponsor within 2 weeks. If their timelines align, there’s a chance that comments will come back from both agencies at the same time. The EMA has also requested that the draft anonymization report is shared before starting anonymization so they can come to an agreement on the approach with the sponsor.
2. Expect Varying Comments
In our first submission preparation, both agencies were open to using one singular anonymization report, however we did notice a few instances of differences in feedback or absence of feedback altogether. We also experienced variance in comments given in the first round of anonymization report vs the second round from the same agency at times. Overall, we received around 5 comments, with more comments from EMA than from Health Canada.
3. Be Prepared to Defend Your Residual Risk Statement
For the draft proposal, we submitted one summary document and patient narratives from one study to show both agencies right away how the client planned to anonymize their narratives. This submission prompted a request from EMA for additional information regarding medical history redactions and how those were represented in our risk simulation calculation and residual risk statement. Our team was able to quickly come back and clarify our process and provide some additional text to the anonymization report about K anonymity along with a reference to show how K anonymity works.
Want to learn more about how data is anonymized? We break it down in an infographic here.
Health Canada did not request any changes at this point but did note that they were supportive of redacting individual participant medical history in the narratives.
4. Sponsor Personnel Names - to Redact or not to Redact?
Health Canada allowed all names (e.g. study administrators or sponsor personnel) to be redacted as personal data, however, according to the EMA in order to comply with Policy 0070 guidelines signatories and principal investigators of the clinical study report (CSR) needed to be released.
5. Align on any Handwritten Dates
Late in the submission process EMA requested that any handwritten dates be redacted and replaced with typed overlay text that reflects the date underneath. Health Canada did not acknowledge the handwritten dates at all. In the end, our team disputed this request due to the tight timeline and lack of inclusion in policy guidance. If you have any handwritten dates in your documents you may want to ask your agency contact ahead of time if they have any preference on keeping them as-is or replacing with an overlay.
6. You may be Expected to use the Agency's Preferred Verbiage
EMA requested different verbiage be used in the anonymization report. This may have been an attempt to standardize terms across published reports. The requested changes were small, e.g. ‘study administrators’ changed to ‘sponsor personnel’. Health Canada was not as particular.
7. Combine Cover Letter Templates for Efficiency
Ask your agency contacts about creating one combined cover letter based on the EMA cover letter template, with the addition of key items from the Health Canada requirements. Consolidating into one letter can help reduce time and documents needed.
8. Use Appropriate Naming Conventions set by Each Agency
Files must be named using the appropriate naming convention for each agency. Both agencies noted that aligning here won’t be possible due to system dependencies on these naming conventions.
9. There's an Additional Labeling Option for Blinding Redactions
Redactions that are necessary to maintain blinding in an ongoing study can be redacted and labeled with "BLD". This method is accepted by both agencies. This information should be included in the anonymization report.
10. Keep Your Justification Tables/Redaction Control Sheets Separate
Justification tables or redaction control sheets are required to communicate proposed commercially confidential information (CCI) along with reasoning for redaction throughout the redaction consultation process. For collaborative submissions, both agencies are still requiring their own respective templates be used, since parameters for CCI or confidential business information (CBI) differ between the two. It's recommended that an initial proposal or discussion about CCI is had with the agency before applying to documents in case of an initial rejection.
Our Biggest Takeaway: Know what you’re doing when you’re calculating risk and be able to defend your methods.
We were able to submit our first client’s package without making document changes to patient information, even though that is where we received the most questions from the EMA. They wanted to know how we conducted the disclosure risk measurement from the reference population, down to the risk threshold and residual risk assessment. If we hadn’t had the level of justification for the methods we applied, it most likely would have been a major headache and more extensive changes may have been needed.
While the EMA did suspend the publication of clinical data in 2018 until further notice, they are publishing clinical data for COVID-19 medicines in line with their exceptional transparency measures for treatments and vaccines for COVID-19. If your organization is not working with COVID-19 treatments or vaccines, you have a bit more time to prepare for collaborative submissions in the future.
Trust the experts to handle your submissions.
d-wise offers outsourced data and document anonymization services utilizing industry-leading Blur anonymization software. Whether your team needs help consistently or intermittently, we’re here to help. Learn more about our software and services here.
